It is late. A caregiver is finally in bed after another day of work, kids, and managing her mother’s medications. The house is quiet. On her mobile device, she opens an email from a new healthcare provider: “Before your first visit, please complete these forms.” She taps the link and lands in a portal she has never seen before. She is asked to create a password—then another one! The site rejects her first choice. She starts answering questions she has already answered twice this year for other providers: date of diagnosis, current medications, fall history, and emergency contacts. The fields are tiny. The drop-downs are finicky on a touch screen (Figure 1). The page keeps scrolling on and on. Nothing about it feels like the beginning of care.
As a product designer, I have heard versions of this scenario more times than I can count from family caregivers, care coordinators, and the clinicians who watch exhausted, defensive people arrive at first appointments. The frustration comes up in primary care, specialist visits, dementia programs, and community services that all genuinely want to do good work. The woman in that scenario is one of nearly 12 million unpaid dementia caregivers in the United States, a group that collectively provided an estimated 19.2 billion hours of care in 2024, and of whom more than half report high or very high emotional stress, per the Alzheimer’s Association. For many of them, the intake form is the first real point of contact.
This article is about the first touchpoint and what those of us who design intake forms can do differently to remove unnecessary friction.
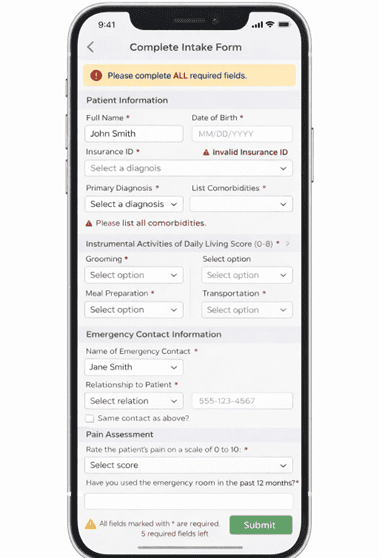
Figure 1: A mobile intake form illustrating the clinical terminology, dense required fields, and scrolling length that characterize many dementia care portals.
The Design Tension
Inside a healthcare organization, an online form is a data pipeline. It produces structured fields that map to a database, satisfy compliance requirements, feed risk models, and populate the Electronic Medical Record (EMR). A good form is one that produces complete, consistent, and queryable data. Data missing from essential fields means yet another phone call. Every incorrect entry can mean a denied claim or a gap in the clinical record.
We add more fields. We split questions up into discrete components so that answers can be scored. We enforce required responses so nothing gets skipped. We add validation rules to protect data integrity. None of the choices is unreasonable on its own. However, together they make the experience feel less like the start of care and more like being processed.
The person on the other end of the form does not experience it as a data pipeline. They are thinking about tomorrow’s appointment, whether they remembered to reorder a blood pressure medication, or whether they are going to break down if someone asks how they are coping. They are wondering whether an honest answer about their own stress might somehow disqualify them from the vital services they need, or whether admitting how much help is needed might make them look like they cannot manage.
What I Learned from Getting It Wrong
When I started building digital intake tools for dementia care, we built forms that were clinically rigorous and practically exhausting. Every section was evidence-based. Every question mapped to a validated instrument or a care planning variable. On paper, these forms were exactly what they needed to be. In practice, caregivers rushed through them, or second-guessed their answers, and sometimes they apologized to staff afterwards for “probably doing it wrong.” One woman told me that she had gone back and changed her answers three times because she was worried she would not qualify for the program if she sounded too capable.
That feedback changed how I viewed the form. It was doing the opposite of what intake is really supposed to do. Instead of helping us understand needs and lighten the burden on a tired caregiver, the form was adding cognitive load and anxiety before the conversation had even begun.
Four Things Worth Doing Differently
Every Label Is a Micro-Interaction
Most clinical intake forms read as though they were written by clinicians for other clinicians to interpret. Terms like instrumental activities of daily living, cognitive status at baseline, and comorbidity burden are precise, but precision is not the same as clarity. When a caregiver has to decode terminology before they can answer the question, they exhaust their mental energy before reaching the questions that actually matter.
Plain language in a form is not about dumbing things down (Figure 2). It is a design decision about who the interface is intended for. For example, “Which everyday tasks do they need help with? …cooking, shopping, managing medicines, or getting to appointments?” conveys the same clinical construct as “instrumental activities of daily living,” but it does not require a glossary to understand it. The same applies to help text, error messages, and section headers. Every line of copy is a micro-interaction. Write it for the person completing the form at 11 p.m., on a phone, not for the analyst running reports the next morning.
Figure 2. An example physical therapy intake form showing contextual “why we ask” language on sensitive questions, human-readable options, and escape hatches for users who don’t have all the information on hand.
Sensitive Questions Need a Reason to Exist
One of the fastest ways to make an intake feel like an interrogation is to ask sensitive questions without any context. A question about emergency service use in the past 12 months, or about the caregiver’s own sleep, is perceived very differently when there is nothing around the question explaining why it matters. Without that context, it is easy to read any question as a trap.
A single line of explanatory copy placed near the question, not buried in a help overlay, but visible in the form, changes the tone completely. “We ask about falls so we can identify safety risks and plan ahead.” “We ask about your sleep because caring for someone with dementia is exhausting. If you are not sleeping well, that tells us you may need more support.” These are not legal disclaimers. They are the equivalent of a clinician explaining why they are asking before they ask. They are also, from a user experience perspective, a straightforward application of progressive disclosure that gives people just enough context to engage with confidence.
Checkboxes Don’t Fit What Needs to Be Said
Structured fields matter, of course. Structured fields make information easier to review, compare, and act on. But a form made only of checkboxes and drop-downs leaves no room for the parts of a person’s situation that do not fit those categories.
“She only recognizes me in the mornings now.” “He still lights up when his old friend visits on Fridays.” “I am terrified of what happens if I get sick.” None of these fits a radio button. But each answer can change how a team understands the person presenting to them. Well-placed free-text fields, such as “Is there anything about your situation you want us to understand?” can surface information that changes how a team approaches the first conversation.
The design decision that matters is not whether to include the field. It is what happens to it on the backend. A narrative field that no one reads is worse than useless; it signals to the caregiver that you asked but did not listen. If you add a free-text question, it must be recorded somewhere that can be reviewed before the first appointment, and someone has to be responsible for acting on what they discover. Build the workflow before you build the field.
The Zarit Burden Interview (ZBI) illustrates where things can get complicated. It is a validated 22-item instrument and an approved dementia care and caregiver support screening tool required by the Centers for Medicare and Medicaid Services (CMS) for their model, Guiding and Improved Dementia Care Experience (GUIDE). ZBI measures a caregiver’s social isolation, emotional strain, and financial pressure. Caregivers, however, often minimize their own distress, sometimes to themselves as much as to anyone else, and a scored form does not change that.
I have been elbow-to-elbow with caregivers, working through the ZBI questions, and have watched them break into tears at questions such as “Do you feel you could do a better job in caring for your relative?” The question is clinically neutral. The intent is to surface self-efficacy and distress. What is perceived in that moment, especially when someone is responding alone on a phone late at night after a long day, can feel more like an accusation. That is not a flaw in the ZBI. It is a reminder that even a well-designed, validated instrument carries emotional weight that its scoring rubric will never capture.
Nobody Should Have to Tell Their Story Four Times
Family caregivers frequently navigate health information across multiple providers and systems, a burden that research has consistently linked to digital fatigue and reduced engagement with care tools. Caregiver portal access has more than doubled in recent years, with the majority of individuals now managing more than one online medical record, per the Office of the Assistant Secretary for Technology Policy in 2025. In my experience, by the time someone reaches a third or fourth intake form, they have stopped writing real answers and started writing shorthand. The cognitive cost of retrieving and retelling the same narrative compounds with each retelling: covering the first symptoms, the crisis moments, and the slow changes compounds an emotional cost.
Inside a single organization, there is no good reason to make someone restate information they have already provided. That means prefilling known data and asking for confirmation rather than re-entry. It means letting people upload a summary document rather than forcing them to retype it into a character-limited field. It means designing shared profiles that span services within a system, not just departments within a form. None of this is technically difficult. It mostly requires the organization to agree that reducing caregiver burden is a design requirement and not just a nice feature.
Figure 3: An intake form using open narrative questions alongside clinical fields, signaling that the team wants to understand the person, not just document the patient.
A Small Change That Had a Larger Effect
After the experience I outlined above, we added a short narrative section to our dementia intake alongside the clinical questions (Figure 3). Instead of only asking about diagnoses and functional status, we began asking questions like “What brings them joy or comfort right now?”, “What does a good day look like for the person you care for?”, and “Is there anything about their background or identity you want us to know?”
These are still form fields, and they can still be mapped to care-planning records. However, they send a very different signal; they tell caregivers that the team wants to understand the human, not just treat the patient.
The change in how people engaged with the form was noticeable. Caregivers slowed down at that section. They wrote about music and morning routines, cultural backgrounds and long-standing fears, and the things that still work even when most things do not. Having that context before a first call can completely change the entire tone of the conversation. Navigators gain a starting point from what matters to this family rather than what matters according to a flat clinical record.
We did not remove the clinical questions. The scores still need to be there. But making space for context inside the same form changed what the form communicated about what we intended to do.
One Test Worth Applying
Before shipping your intake form, ask yourself one question: “Would this feel respectful at 11 p.m. on a bad day, on a phone, and in a tired person’s hands?”
It is a simple heuristic, but it is harder to pass than it sounds. Digital information collection that satisfies the data model, passes validation, and delights the analytics team can still fail this test completely. And if it fails, the person who taps the form’s link for the first time, placing a small amount of trust in the organization before they have met anyone there, will know it within 30 seconds.
Such consideration of the emotional impact matters beyond the experience of one tired caregiver. High caregiver burden is consistently associated with higher rates of emergency department use and earlier institutionalization. A 2019 randomized trial of the Care Ecosystem dementia care model found that when caregiver burden was identified and addressed early, emergency department visits fell and total Medicare costs dropped by an average of $526 per patient per month. The intake form is often where the burden first becomes visible or is overlooked.
Forms are usually the easiest thing to fix. The harder work is getting organizations to care about what happens to the answers. But that is exactly the work worth doing.
Resources
Alzheimer’s Association. 2025. “2025 Alzheimer’s Disease Facts and Figures.” Alzheimer’s & Dementia 21 (4): e70235. https://doi.org/10.1002/alz.70235.
Bispo Júnior, J. P. 2022. “Social Desirability Bias in Qualitative Health Research.” Revista de Saúde Pública 56: 101. https://doi.org/10.11606/s1518-8787.2022056004164.
Centers for Medicare & Medicaid Services. 2024. Guiding an Improved Dementia Experience (GUIDE) Model. U.S. Department of Health and Human Services. https://www.cms.gov/priorities/innovation/innovation-models/guide.
Greenhalgh, Trisha, and Brian Hurwitz. 1999. “Narrative Based Medicine: Why Study Narrative?” BMJ 318 (7175): 48–50. https://doi.org/10.1136/bmj.318.7175.48.
Guo, H. J., and A. Sapra. 2022. Instrumental Activity of Daily Living (IADL). PubMed. StatPearls Publishing, November 14. https://www.ncbi.nlm.nih.gov/books/NBK553126/.
Guterman, E. L., R. E. Kiekhofer, A. J. Wood, I. E. Allen, J. G. Kahn, S. Dulaney, J. J. Merrilees, et al. 2023. “Care Ecosystem Collaborative Model and Health Care Costs in Medicare Beneficiaries with Dementia: A Secondary Analysis of a Randomized Clinical Trial.” JAMA Internal Medicine 183 (11): e234764. https://doi.org/10.1001/jamainternmed.2023.4764.
Kitwood, Tom. 1997. Dementia Reconsidered: The Person Comes First. Open University Press. https://doi.org/10.1136/bmj.318.7187.880a.
Nielsen, Jakob. 2006. “Progressive Disclosure.” Nielsen Norman Group, December 3. https://www.nngroup.com/articles/progressive-disclosure/.
Office of the Assistant Secretary for Technology Policy. 2025. Individuals’ Access and Use of Patient Portals and Smartphone Health Apps, 2024 (Data Brief No. 77). U.S. Department of Health and Human Services. https://healthit.gov/data/data-briefs/individuals-access-and-use-patient-portals-and-smartphone-health-apps-2024/.
Possin, Katherine L., J. J. Merrilees, S. Dulaney, K. Lee, W. Chiong, S. M. Hooper, R. Kiekhofer, et al. 2019. “Effect of Collaborative Dementia Care via Telephone and Internet on Quality of Life, Caregiver Well-Being, and Health Care Use: The Care Ecosystem Randomized Clinical Trial.” JAMA Internal Medicine 179 (12): 1658–1667. https://doi.org/10.1001/jamainternmed.2019.4101.
Santana, S., J. N. Burdine, J. K. Benz, J. Cerully, C. Davey, C. F. Garfield, D. Glik, et al. 2021. “Updating Health Literacy for Healthy People 2030: Defining Its Importance for a New Decade in Public Health.” Journal of Public Health Management and Practice 27 (6): S258–S264. https://doi.org/10.1097/PHH.0000000000001324.
Sweller, John. 1988. “Cognitive Load During Problem Solving: Effects on Learning.” Cognitive Science 12 (2): 257–285. https://doi.org/10.1207/s15516709cog1202_4.
Wolff, Jennifer L., J. D. Darer, and K. L. Larsen. 2016. “Family Caregivers and Consumer Health Information Technology.” Journal of General Internal Medicine 31 (1): 117–121. https://doi.org/10.1007/s11606-015-3494-0.
Zarit, S. H., K. E. Reever, and J. Bach-Peterson. 1980. “Relatives of the Impaired Elderly: Correlates of Feelings of Burden.” The Gerontologist 20 (6): 649–655. https://doi.org/10.1093/geront/20.6.649.
Zhai, S., F. Chu, M. Tan, N.-C. Chi, T. Ward, and W. Yuwen. 2023. “Digital Health Interventions to Support Family Caregivers: An Updated Systematic Review.” Digital Health 9: Article 20552076231171967. https://doi.org/10.1177/20552076231171967.

Ollie Fielding is a product and technology leader focused on designing digital tools that make healthcare easier to navigate. As co-founder of Lizzy Care Inc., he builds products that support families and caregivers managing dementia and complex care needs. His work centers on human-centered design, using technology to simplify care journeys and improve everyday health decisions.
User Experience Magazine › Forums › Designing Forms for Tired Caregivers: Decreasing Digital Fatigue