Old age is a natural stage in life. According to statistical studies, societies are aging at an increasingly rapid rate; in 2060, the number of aged people in European countries will double. According to M. Kawińska, a significant portion of them will be people who require continuous or periodic medical care.
The body regulating the patient care process is the healthcare system. The most frequent solution to a situation in which continuous patient care is required is a hospital procedure associated with a temporary stay.
However, there do exist systems that base their operations in considerable measure on care outside the hospital setting. One such system operates in Switzerland, a country with a unique healthcare system that is largely based on the activity of Spitex non-government organizations (from “Spitalexterne Hilfe und Pflege,” meaning out-of-hospital aid and care).
The very premise of this system is based on home care and the activity of nurses who, aside from working with the patient, often play the role of managers, assistants, and liaisons among the patient, the patient’s family, the doctor, and the hospital.
Context
Historical and Community Background
The medical care system in Switzerland is connected to the genesis of the state, or properly speaking, the confederation of states. Despite historical connections (some of which have existed for over 700 years), states have retained their independence and ability to decide about legal regulations within a given canton.
The beginnings of the first Spitex organization date back to the year 1857 when the position of community nurse was officially created in Zürich. Their fundamental role was to provide medical care and aid, as well as organizational support to patients living within the canton. In 1882, the canton of Zürich formally created an organization that was the first public institution whose only task was to provide healthcare to the local community.
Mobile Hospital
The key to understanding the challenges faced by nurses working in Switzerland in current days is the care model; it is the service provider who goes to the home of the patient and provides services in the surroundings that the patient knows. The most frequent case is a situation in which a patient, after being signed out of the hospital and provided with the attending doctor’s prescription for Spitex organization services, returns home with the basic medical materials essential for the first few days of convalescence.
The next day, a nurse appears at the patient’s home, takes a nursing history, and establishes a care plan (Pflegeplan). At the same time, the nurse provides basic care and teaches the patient how to bandage postoperative wounds. In doing so, the nurse makes use of medical materials brought along for that purpose.
This recalls the manner in which nurses worked in the 19th century, carrying with them a medical bag with nursing materials (Pflegetasche) by bicycle. This bag became the identifying mark of Spitex nurses and, despite being a backpack today, still functions in community consciousness as their attribute.
The Role of the Nurse
One thing that differentiates Switzerland’s healthcare system from other systems is the influence of the nurse on the medical care process. What might be considered the subordinate position of nurses relative to doctors, often visible in other countries, has no raison d’être here. It is the attending nurse who bears the greatest measure of responsibility for the convalescence process; in doing so, the nurse carries out diverse functions from the typical ones associated with providing medical aid and care to managing contact with the doctor, ordering medical products from the pharmacy, and cooking or cleaning in the patient’s home.
Case Study
An e-service must maintain home care as its core value yet cover the aspects of managing the patients while keeping the service scalable. The re-design of the application accounted for an expanded e-store with additional functionalities, medical materials delivery planning, settling accounts and documenting medical materials used per legal regulations, and scaling to different population concentrations.
Challenges to overcome included inconsistent access to infrastructure, organizational differences based on the number of nursing staff, multiple language requirements for the interface, business structures that hampered standard user testing, and the remote aspect of the work as the whole service was designed and developed by external employees, none of which were Swiss residents.
Scope of Work
 Figure 1: The medical materials e-store interface before the start of design work.
Figure 1: The medical materials e-store interface before the start of design work.
The previous service was initially an e-store with over 6,000 products, among which nurses were supposed to choose which, in their opinion, would best serve the patient in a quick return to health. Since 2016, it had worked on a B2B model (and later B2B2C). B2B (business-to-business) is a business model that assumes collaboration between two companies. The B2B2C (business-to-business-to-consumer) model additionally includes the end customer, in this case, the patient. Spitex organizations order medical materials via an e-commerce platform, and the product is delivered directly to the patient’s home or (in the case of specialized materials) to the Spitex warehouse, from which nurses later transport materials in the medical bag (Pflegetasche) to a specific nursing visit.
Over time, the e-store expanded with additional functionalities resulting from organizational needs, such as automatic deliveries, a medical material usage plan, and a warehouse inventory tool. In this version, the main emphasis was on the visualization of product categories designed as extensive trees of sub-categories. It became problematic to manage choices and search for products.
The legal regulations in Switzerland also require a suitable system to settle accounts and document the medical materials used. A key component was to facilitate documentation of the fact of material usage by a specific patient and to make appropriate plans for the patient’s future usage. Service support took place with the participation of the Solution Center, a unit specializing in provision of information, acceptance of telephone orders, and servicing of returns.
My role was to redesign the e-service for these purposes so that its main focus was the patient and the patient’s needs, not products and procedures.
Challenges and Barriers
To properly understand the scope of the problem, one must understand the limitations and barriers that impacted the solution used in the new design. These can be divided into the following barriers:
- Infrastructural
- Technological
- Design
- Cultural
Infrastructural
To this day, the operational model of the Spitex organizations consists of providing support to local communities.
Because of large differences in population density within Switzerland and its division into cantons, active units cover both agglomerations where population density exceeds 1,000 persons per km2 and within cantons comprised of small villages.
Population concentrations are located in the northern and northwestern portions of the country, but medical care is required by all communities within the cantons, including those with less population density. This division directly impacts the way that nurses work in each locality.
This difference necessitated a design that would be scalable and adaptable to the needs of organizations of differing sizes. Spitex organizations can be institutions with thousands of patients, management teams, and a numerous, qualified nursing staff, but in less populated areas, the same type of work is performed by one nurse, caring for a few patients.
 Figure 2: Population concentration impacts different localities’ organizational needs.
Figure 2: Population concentration impacts different localities’ organizational needs.
Technological
The geographical situation of Switzerland affects the signal quality of the telephone and Internet network. In Switzerland itself, there are many places in which the signal is so weak that it is impossible to maintain continuous Internet access. An important element of the design is to ensure continuous access to full-service functionality. A stable solution includes offline-capable e-service that enables realization of tasks in offline mode and synchronization at moments of access to a stable network signal.
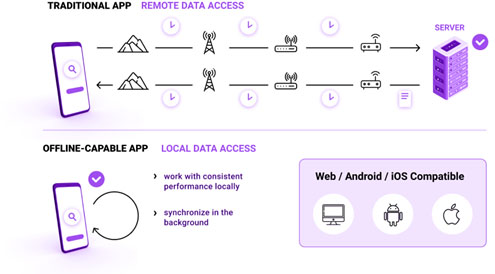 Figure 3: A considerable portion of e-services assumes continuous Internet access, which can cause delays in data transmission via many intermediate points.
Figure 3: A considerable portion of e-services assumes continuous Internet access, which can cause delays in data transmission via many intermediate points.
Offline activity increases the risk of warehouse shortages. Imagine a situation in which a nurse orders specific products for a patient without access to online service. During the return to full online mode and synchronization with the server, it can turn out that the product ordered was meanwhile bought by another organization.
Such an operational model requires the existence of a customer service support unit in a firm’s structure. In this case, this function is served by the Solution Center, the team supporting organizations at the individual stages of the service operation, for example, during the purchasing process.
Design
The proper execution of the design process assumes access to end users and must thoroughly account for the needs and problems that they encounter. Because of the great dispersion of Spitex organizations and diversity of ways in which these institutions work, it is not possible to prepare one model on which to base the service structure.
The entire technology team responsible for the development of the service worked in remote mode. In the initial phase of the project, I was responsible for the user experience area; in later phases, two more designers (from Spain and Poland) joined the team. The fundamental design challenges were associated with preparing methods to enable collaborative design work as well as determining channels and methods of communication among teams.
Another challenge was the way that the service operates; the B2B2C model became a barrier to the designers’ access to users (that is, to nurses working with Spitex organizations) as well as to patients due to confidentiality requirements for medical information.
Cultural
Cultural differences within the Spitex organizations themselves created a barrier. We prepared the e-service for three of the official languages in Switzerland: German, Italian, and French. This gave rise to design challenges with the internal construction of the language and with predicting the manner in which the service should adapt itself to the requirements of a given language.
For example, Italian and French display considerable structural similarity (both are Romance languages), which theoretically facilitates design of content comprised of texts; however, German, which uses compound words and a different grammatical construction, requires solutions that account for the impossibility of dividing words or interface elements that must display optimally on the device screen regardless of the language.
The Design Process
Methods and Procedures
The 1970s, with the first personal computers and the development of the Human-Computer Interaction field, started the process of working out user experience design methods. Today, digital artifacts are full-fledged products in the same sense as the design of a teapot or a book.
The final quality of the proposed solution is influenced by methods permitting empathy with the user of a given product or service; the designer must understand the user’s needs. There is a visible shift in decision-making from individual persons to teams, as well as closer contact with the product’s end user via focus-group interviews, surveys, in-depth interviews, and in the case of UX designers, via prototyping early digital product solutions and verifying them in usability tests.
In the software design process, several methodologies are used that support its realization. The most often-used software development methodologies are these:
- The cascade model assumes a sequential execution of work in which successive stages are executed after completion of previous ones.
- The spiral model assumes a repeated spiral or progression through determination of premises, assessment and risk reduction, implementation and evaluation, and successive phase planning.
- The RUP (Rational Unified Process) model distinguishes four phases of the software life cycle: Inception, Elaboration, Construction, and Transition. These phases refer to successive business processes connected with the project execution stages.
- The agile model is based on rapid reaction to a changing work environment and assumes multiple returns to each of the phases, together with changing requirements and an increasing store of knowledge about the user and usage processes.
Presently, the most often-used models are based on an iterative approach and agile methodologies. The phases of the design are closely connected; however, they are not based on a linear structure (from the information-gathering phase through the implementation phase), but on loops that assume multiple returns to the phases of previously defined assumptions, design, user tests, and support after implementation of the e-service.
The e-service’s design was premised upon the application of agile methods. The service has been designed as an application operating in an Internet browser environment, enabling access regardless of the operating system and model of the device owned by users.
Work Environment
Choosing tools for a remote team takes on fundamental significance. These tools should facilitate designers’ gathering and interpretation of data, as well as enable them to share knowledge within the design team, among the programming teams, and with the project managers.
Our solution was a cloud-based environment, in which each participant in the design process can view, comment upon, or edit the shared data depending on authorizations. This method considerably speeds up execution of the work, especially for a team comprised of people living in different time zones. In this way, it is possible to design the successive modules of the system and simultaneously manage the project, including checking the compatibility of the design with its implementation.
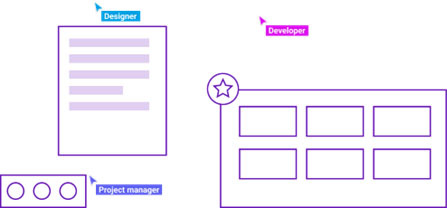 Figure 4: Execution of the project in an online environment enables people to work simultaneously on different modules of the service.
Figure 4: Execution of the project in an online environment enables people to work simultaneously on different modules of the service.
The Role of Internal Consultants
In a typical design process, it is assumed that data can be gathered with the aid of analytical tools or research methods.
In this design, data were not gathered beforehand but gained through the knowledge of the Solution Center. A number of people in support operations indicated that the existing e-service was not serving its purpose properly. A logical step was to attempt to gain data via the people working in the customer service department.
The risk associated with internal consultants is working with information subject to multiple interpretations. The designer’s responsibility is to construct the interview formula to understand what problem was reported, how it was resolved, and what its real cause could have been.
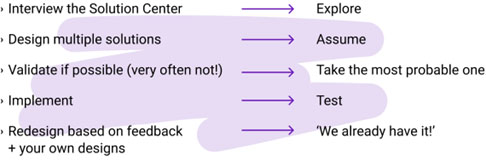
The Educated Guess Method
It was impossible to test solution prototypes with user participation. The complex nature of the modules, such as the prescription creation tool, also generated organizational problems. The amount of time required to prepare a credible solution prototype slowed the design process so much that it was necessary to work out an alternative method.
In a typical user experience design process, usability tests are often carried out on low fidelity mock-ups that can be quickly discarded if a concept is found to be ineffective. Low fidelity mock-ups are views of the interface of individual e-service use stages with low visual fidelity, often in sketched-out form. However, especially in organizations with no previous experience working with a user experience designer and in a project that was entirely remote, low visual fidelity suggested low design quality.
Therefore, the proposed method (educated guess) consisted of an analytical process using the iterative approach and agile methods with research gathered from internal consultants. The knowledge gained served to work out hypothetical models of user behavior to develop an assumed user journey. More than a dozen possible use processes were designed to serve the same purpose, such as ordering medical materials, in a high-fidelity interface.
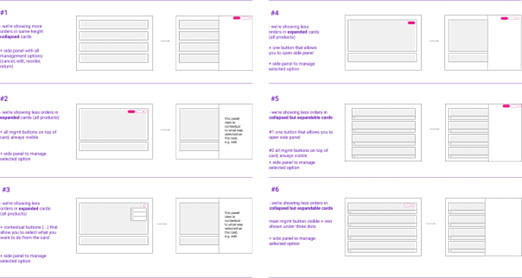 Figure 5: Initial concepts for a low-fidelity view of the Order History section.
Figure 5: Initial concepts for a low-fidelity view of the Order History section.
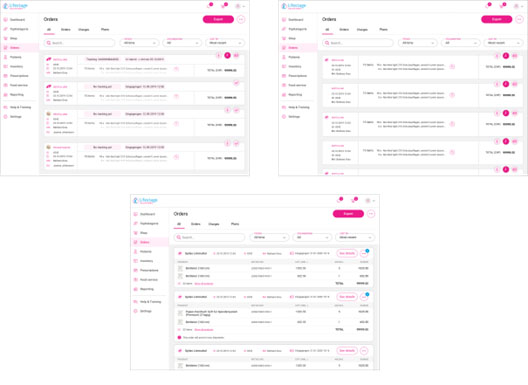 Figure 6: Concepts for a high-fidelity view of the Order History section.
Figure 6: Concepts for a high-fidelity view of the Order History section.
The usability test phase was omitted; the selected solution was implemented based on team decision and on knowledge gained from people working in various departments of the company. The high risk of failure associated with a design process carried out in this manner was minimized as much as possible by consultations with internal experts on their collective knowledge.
In some situations, this method did not work, especially if design decisions were made based on insufficient knowledge of the real use process. Requests for changes in the way that individual e-service modules operated were often reported by individual organizations, but because of the different ways the organizations work, it was not possible to assume that the same solution would be equally effective in other organizations. A hypothetical behavior model was applied instead. In many cases, the proper solution had already appeared during the design work phase but was rejected for business or utility reasons.
Returning to previously prepared interface versions made it possible to shorten the time to new solutions. Feedback served to verify design concepts, and the high visual fidelity of the hypothetical solutions enabled implementation documentation to be prepared quickly (sometimes even in a few hours).
This method was slow in the initial stages of a project; it was necessary to predict possible use situations in advance and design variants thereof. The longer concept phase, however, permitted the time needed to carry out the implementation phase of the project. The ability to make changes very quickly at this stage can support the building of a positive relationship with the customer.
Experience
This method had weaknesses: There is a limit to the solutions that can be proposed relying exclusively on presumable scenarios. The designer is faced with the necessity of determining which of the proposed solutions should be implemented; but without knowledge of the real medical care process, each of them is equally probable.
One method frequently used in the initial phases of a project (the information gathering process) is participatory observation. In this case, carrying this out became possible only after eight months of work on the project.
Observations carried out in January 2020 consisted of:
- Participation in the process of creating medical documentation by a nurse specializing in work with patients with psychiatric disorders;
- Observation of the organization management process (planning of shifts, determination of vacation schedules, documentation, and settling of accounts for time worked);
- An interview with a person responsible for planning nursing visits;
- An interview with a person who manages the patient registration process; and,
- Observation of the medical care process during a nursing shift.
The observations showed that the most important aspect for all persons involved in the patient care process is effectiveness. The persons observed were able to perform even complex tasks in unfavorable conditions (the nurse acquainted himself with the patient’s medical documentation after arriving at the place of residence, in the car shortly before the visit). The problematic areas indicated were these: the illogical structure of the application, difficulties in searching for medical products, and a complicated process for creating medical documentation using a mobile device.
For designers, observed experience becomes the main factor serving to verify the sensibility of the designed solutions in the later stages of work.
E-Service Scalability
In the solution designed, scalability was understood as the service’s ability to adapt itself to the needs of organizations of varying size to best serve its intended purposes.
This was achieved through the application’s modular construction. Each organization, at the service configuration stage, can decide which modules are essential to their basic medical care tasks.
The focus of the service is always an e-store with medical products, but several services co-exist to support nursing care: delivery planning based on usage of materials, a prescription management module, a catering service, a warehouse inventory module, and a cyclical order module. As part of the service, Spitex organizations also have access to a business module that permits them to monitor basic economic indices in the organization.
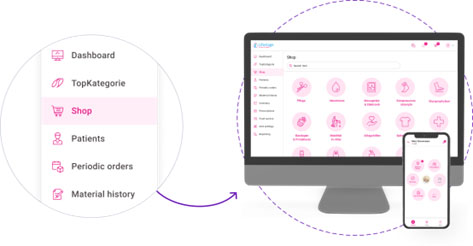 Figure 7: Modular application interface structure in the re-designed version in which the medical materials store is one section of the e-service.
Figure 7: Modular application interface structure in the re-designed version in which the medical materials store is one section of the e-service.
The medical materials store is a section in the e-service, which permits the interface to be easily adapted to the needs of individual organizations. Organizations can allow access to the full functionality of the service or purposely narrow it.
An additional module is a mobile application intended for nurses. The scope of available functionalities has been purposely limited, and is intended, to facilitate the process of working with a patient. The module focuses on the patient’s needs, without necessitating access to administrative processes.
A key aspect of the application is a context-aware design approach, which provides the user appropriate content when that content is needed. To achieve a context-aware design, we used technological solutions such as a GPS and a smartphone camera.
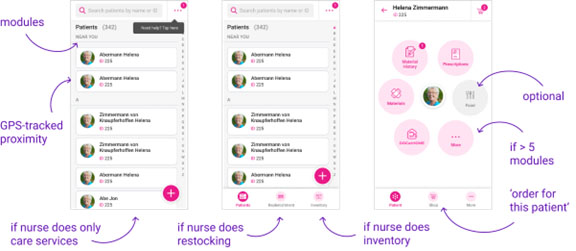 Figure 8: Different versions of the mobile application for nurses (left: simplified version; center: expanded version for organizations managing and carrying out warehouse inventory processes; right: patient as the focal point surrounded by available services).
Figure 8: Different versions of the mobile application for nurses (left: simplified version; center: expanded version for organizations managing and carrying out warehouse inventory processes; right: patient as the focal point surrounded by available services).
Non-Standardization
To ensure a high-quality product, relevant norms and regulations serve as a point of reference in the design process. Standardization in user experience design can refer to research methods, the process of working through successive stages, and to concrete design solutions called standards. These standards concern the principles of operation, the logical construction, or the visual aspect of interface elements. They function in the form of both norms (ISO 9241-110:2020) and best practices available online in article form.
In the redesign, these principles found only partial application. The scale of the project and the necessity of combining such different service elements required solutions that—according to an assessment in terms of current norms—could be considered wrong.
One such solution is the Cart, an interface element that should have a clearly determined structure. The metaphor of adding products to the cart reflects the real world; it refers to customer buying habits and is a standard solution in the e-commerce field. In the existing service, there were two independent carts. Nurses could add products to one shopping cart that were to be delivered to the client by courier, or they could add products to a different cart which they would bring with them during a nursing visit.
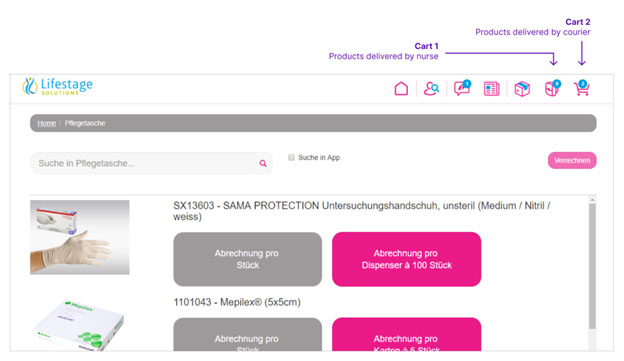 Figure 9: Two carts before the re-design for products delivered by courier versus products delivered by nurse.
Figure 9: Two carts before the re-design for products delivered by courier versus products delivered by nurse.
This solution was supposed to facilitate the division between the products that the nurse ordered versus the products that the nurse used. This solution did not work properly. Nurses often confused the carts, looking for chosen products in the wrong place.
The solution was to integrate the two functions into a single Cart. Separate sections enabled the nurse to check and correct the order without the need to switch back and forth between different carts.
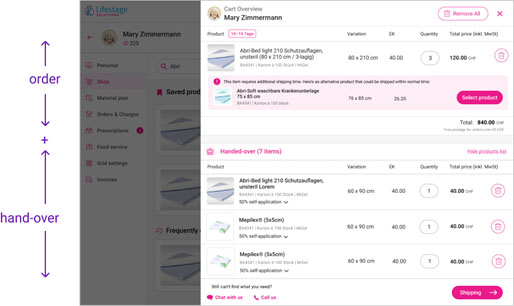 Figure 10: Shopping cart in side-panel form.
Figure 10: Shopping cart in side-panel form.
An important aspect of the Cart was to emphasize the context of ordering for the patient while at the same time achieve a feature that would be easy to use for tracking which materials were given to the patient. Additional facilitations included the estimated delivery date and alternative products (cheaper or more quickly available) that could be exchanged in a simple manner for others in the same cart.
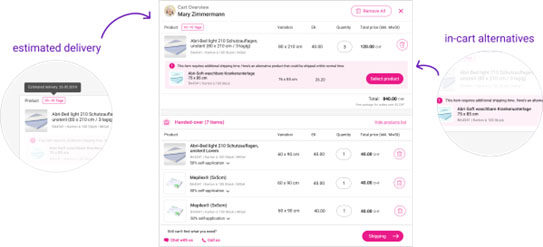 Figure 11: The cart divided into two sections: Order (upper section) and Handed-over (lower section).
Figure 11: The cart divided into two sections: Order (upper section) and Handed-over (lower section).
Another departure from the standards was the design of the prescription management tool. According to commonly accepted principles, division into sections is used for situations in which the user shifts between interface views for a given context. The important thing is that the function of the sections is similar.
In this case, the solution was determined by the quantity of data that a nurse inputs. Each section can be filled out separately; some are not required. The element that brings the sections together is the side panel.

Figure 12: Prescription creation panel (left: patient personal data; center: indication of illness authorizing the prescription to be issued; right: list of product categories in accord with state MiGeL (Mittel- und Gegenständeliste) medical materials list).
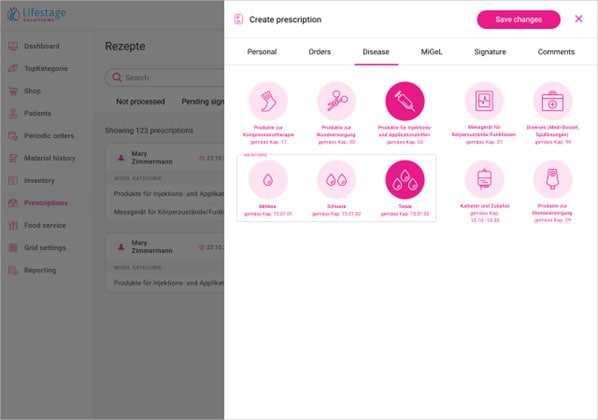 Figure 13: Section listing the most common illnesses authorizing a prescription to be issued.
Figure 13: Section listing the most common illnesses authorizing a prescription to be issued.
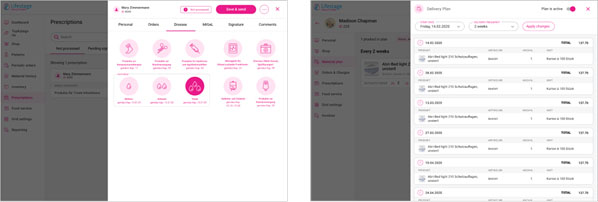 Figure 14: Example of the application with the same interface mechanism concept in two different situations. The operation of the interface elements is the same in both cases (pull-out side panel), but their purpose is different (left: prescription management panel; right: delivery plan management panel for a specific patient).
Figure 14: Example of the application with the same interface mechanism concept in two different situations. The operation of the interface elements is the same in both cases (pull-out side panel), but their purpose is different (left: prescription management panel; right: delivery plan management panel for a specific patient).
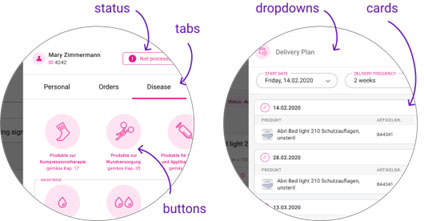 Figure 15: Set of interface elements, enlarged.
Figure 15: Set of interface elements, enlarged.
This article includes only a few of the many examples of solutions that were designed. Conscious departure from commonly accepted norms is risky but can also bring solutions that—despite theoretical disagreement with the standards—still work.
Summary
The dynamic changes of the labor market require considerable elasticity from teams working on new products and services. What becomes key to the success of a design is openness to non-standard solutions, both in methods used and concrete design solutions.
What remains a challenge is to design methods of collaboration among all parties involved in the project. Non-standardization should not only serve to increase effectiveness and optimize processes; its role is, above all, to assist in seeing the center of these processes: the human being.

Kamil Kamysz teaches as an assistant professor in the Faculty of Industrial Design at the Jan Matejko Academy of Fine Arts in Kraków. Currently, he leads a UX team executing projects for the health service sector in Switzerland as a UX designer at Toptal.com. He specializes in the design of complex digital products.